This study investigated the significance of
LASI, LAVI, AEMD, and LAKE indicators of left
atrial electromechanical function as stroke markers
in patients with micro-AF. Although there is a
significant body of studies on stroke in patients with
AF, these markers have not been studied before in
a group of patients with micro-AF. Patients with
atherothrombotic occlusion, lacunar infarction, and
transient ischemic attack were also not included in
our study, whereas patients with a high probability of
cardioembolic stroke were included.
In a cohort study of ablated AF, the LA sphericity
index was found to be an independent risk factor for
arrhythmia recurrence.[7] In another study, patients with
more spherical LA also had a more frequent history of
thromboembolic events.[13] In a different study, healthy
patients with 30 or more supraventricular ectopic beats
had a three-fold increase in AF prevalence and a 60%
increased risk of stroke and death after 6.3 years.[9] In
the study by Tove Hygrell et al.,[14] the micro-AF group
also had the highest cumulative incidence of stroke
(4.1%) and death (10.3%). In previous studies, the
prevalence of AF was found to be more than four times
in the micro-AF group (13%) compared to the control
group (3%).[7] Increasing LA pressure and volume for
various reasons causes changes in LA shape.[11] The
LA tries to provide optimum volume/surface area by
becoming more spherical as an adaptation mechanism
to reduce wall stress. Increased LA pressure expands
the atrium along the atrial orthogonal axis, causing the
shape of the atrium to change from oval to spherical.
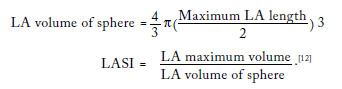
Since the LA expands by different amounts in
the three-dimensional plane, the LA volume and
sphericity index can measure LA dimensions more
accurately than linear measurements of LA.[11]
Methods such as MRI and cardiac CT are invaluable
for assessing asymmetric changes in LA.[11] However,
the radiation exposure and time-consuming nature
reduce the usability of these processes.
We observed that a higher LASI and LAVI,
which means a more spherical LA, increases
the risk of stroke. Therefore, close follow-up of
patients with micro-AF with high LASI and LAVI
in terms of stroke is essential. Deconstructed LA is
more prone to the development of AF.[7] Left atrial
kinetic energy, which is an important indicator
of LA mechanical function, also decreases over
time. Left atrial kinetic energy has been observed
as a predictor of AF recurrence, independent of
the LA diameter.[7] This proves that it is wrong
to evaluate LA function by LA diameter alone,
While electrical remodeling starts early in the AF
process in the atria, structural remodeling is a late
histopathological manifestation.[7]
The duration of AEMD is closely related to
the histopathological changes in the atrium.[12] In
particular, as reported in previous studies, the delay
time in this conduction is greater in the lateral walls
of the LA and left ventricle, which are further away
from the sinus node.[7,15,16] Park et al.[15] found left atrial volumes and AEMD durations to be longer in patients
with AF recurrence, supporting our study. In the study
of Osmanagic et al.,[16] when the LASI value was taken
as 0.9, the specificity was 79.3% and the sensitivity
was 51.8% in predicting AF recurrence. Similarly,
LASI was significantly higher in stroke patients
with micro-AF in our study (0.78±0.05 in Group 1
vs. 0.67±0.04 in Group 2; p<0.001). It is important
to provide rhythm control in the early period to
prevent LA geometric remodeling and cardiovascular
events that may occur due to AF. Predictors such as
AEMD, LASI, LAKE, and LAVI will help us in
early diagnosis before AF becomes permanent. In our
study, we emphasized the importance of these indices
in predicting stroke risk in patients with micro-AF.
How AF burden affects stroke risk is an ongoing
discussion. A meta-analysis of studies in patients not
using oral anticoagulant (OAC) therapy shows that
patients with more persistent forms of AF rather
than paroxysmal have a higher risk of stroke.[17] Atrial
fibrillation progresses from the paroxysmal form to
more permanent forms over time, and this situation
increases with increasing age.[18] It is not known if
high-risk individuals with micro-AF would benefit
from OAC. However, these patients may benefit from
risk-free interventions, primary prevention, optimizing
lifestyle factors, and treating comorbidities as an effort
to reverse atrial myopathy.
In the study by Binici et al.,[9] healthy individuals
aged 55 to 75 years who underwent 48-h ECG
monitoring were analyzed for supraventricular
tachycardia (≥20 beats) and ≥30 supraventricular
ectopic beats per hour. At the 6.3-year follow-up, they
found a three-fold increase in the risk of developing
AF and a 60% increase in the risk of death compared
to the control group. It was determined that the
number and duration of supraventricular beats were
directly proportional in the development of AF.
According to this study, OAC should not be started
in patients with micro-AF and low supraventricular
beats with a high risk of bleeding. In a Swedish
cohort study, individuals free from AF were followed
prospectively for >13 years.[19] Irregular SVTs without
P waves showed the strongest association with clinical
AF, with a cumulative incidence of 47.4%. Judging by
studies and meta-analyses, there is no consensus on
the treatment approach in patients with micro-AF.
Oral anticoagulant therapy may be started in patients
with micro-AF with a high CHA2DS2-VASc score,
but prospective comprehensive studies are needed. Comprehensive multicenter studies to be conducted
in the future may lead to early initiation of medical
treatment in patients with early AF risk. Therefore,
these predictors are important in diagnosis and
follow-up.
There are several limitations to this study. First,
it was a single-center retrospective study with a
small number of patients. Due to limited number of
patients, the study cannot be attributed to the entire
population. Second, there was a difference between
the two groups in terms of the number of patients.
Additionally, cardiac MRI and CT methods could
be used in addition to TTE for LAVI and LASI
calculations in patients with poor image quality.
Lastly, longer Holter monitoring or a loop recorder
could be fitted for patients with micro-AF on 24-h
Holter recordings to detect paroxysmal AF attacks.
In conclusion, early diagnosis and treatment of
micro-AF, which is the predictor of AF in the
long term, is crucial. We can identify and treat
these patients who are at risk of cardioembolic
stroke with easily calculable indices. These new
parameters may contribute to other parameters, such
as CHA2DS2-VASc score and atrial diameters, in
predicting cardioembolic stroke.
Ethics Committee Approval: The study protocol was
approved by the Tekirdağ Namık Kemal University Ethics
Committee (date: 28.12.2021. no: 2021.283.12.06). The
study was conducted in accordance with the principles of the
Declaration of Helsinki.
Patient Consent for Publication: A written informed
consent was obtained from each patient.
Data Sharing Statement: The data that support the
findings of this study are available from the corresponding
author upon reasonable request.
Author Contributions: Idea/concept, data collection
and/or processing, analysis and/or interpretation, literature
review, writing the article, materials: C.A.; Critical review,
references and fundings, control/supervision: M.E.
Conflict of Interest: The authors declared no conflicts
of interest with respect to the authorship and/or publication
of this article.
Funding: The authors received no financial support for
the research and/or authorship of this article.




















){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}